POUR Algorithm
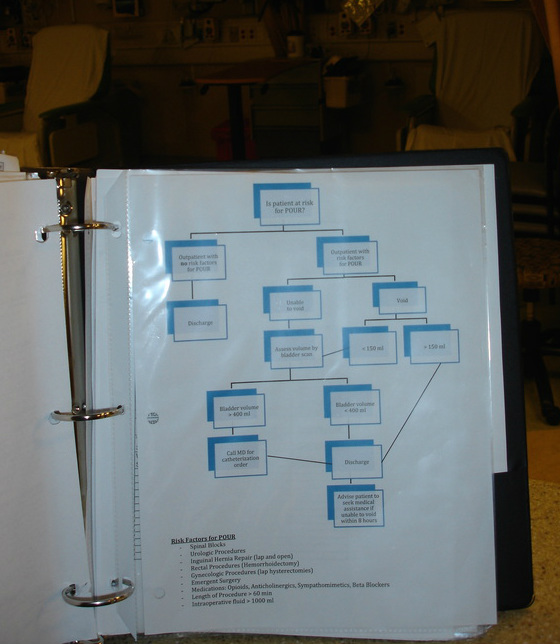
Based on the literature, I created a voiding algorithm to use as a guideline, which would require patients at a high risk for POUR to void a certain amount prior to discharge. If unable to void or voiding less than 150ml, the nurse bladder scans and contacts the surgical team for further orders (i.e. straight catheterization, Foley catheterization, or discharge).
After presenting the voiding algorithm to PACU nurses in the October staff meeting, nurses began implementation in Phase II (the discharge area).
After presenting the voiding algorithm to PACU nurses in the October staff meeting, nurses began implementation in Phase II (the discharge area).
The voiding algorithm was placed in the Phase II binder
making it easy to reference.
making it easy to reference.

|
I noticed that the bladder scanner was in the Phase I utility room. This meant that in order to bladder scan, a nurse had to leave the Phase II area and take a long walk to the Phase I utility room. Many times, a nurse or CNA would not be available to watch his/her patients while collecting the bladder scan. It was not a safe situation.
Following managerial approval, I moved the bladder scanner to the Phase II utility room closest so that PACU nurses could easily and safely access it. |
|
Nurses also reported that it was difficult to measure urine output because hats and urinals were not readily available. To remedy this problem, the PSC and I located an unused file cabinet, filled it with hats and urinals, and placed it in the Phase II bathroom. Now, measuring output is within arm's reach.
|

|
Click to return to POUR Implementations
