Provider's Perception
In August 2013, I informally surveyed surgical attendings, surgical residents, anesthesiologists, anesthesia residents, and Certified Registered Nurse Anesthetists. I asked them if they thought ALL outpatients voided prior to discharge home from PACU.
It's important to note that voiding prior to discharge was not a PACU standard. Patients only voided if the surgical provider wrote a nursing communication order stating that patient must void prior to discharge.
It's important to note that voiding prior to discharge was not a PACU standard. Patients only voided if the surgical provider wrote a nursing communication order stating that patient must void prior to discharge.
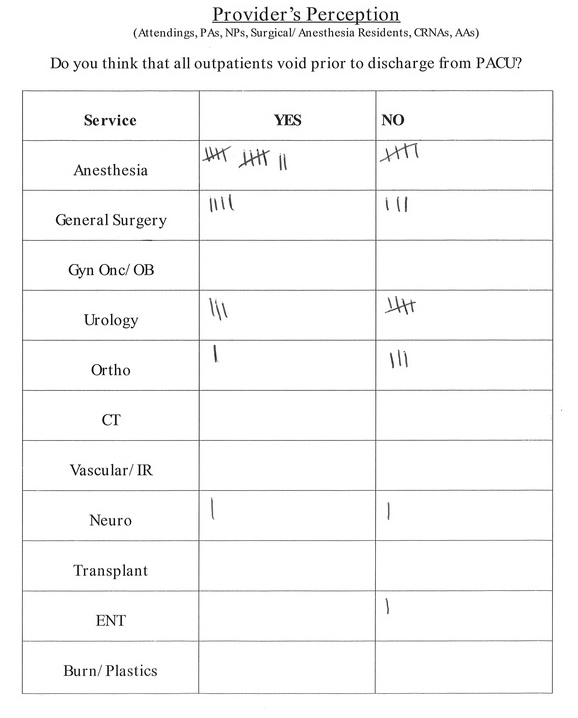
21 out of 39 providers (54%) assumed that patients voided prior to discharge.
T
he biggest discrepancy was among the anesthesia service. 12 out of 17 (70.6%) anesthesia providers assumed patients voided prior to discharge. Whereas, 9 out of 22 (41%) surgical providers assumed the patient voided prior to discharge. After studying the risk management case where the patient was readmitted with POUR, I learned that the nurse was exclusively communicating with the anesthesiologist.
In PACU, the nurse has to decipher if he/she should communicate an issue with the surgical team or anesthesiologist. The vast majority of issues are anesthesia-related, meaning the nurse defers to the anesthesiologist. However, POUR is multifactorial and the biggest contributor to increased risk is the type of surgery. Furthermore, the survey highlighted a lack of knowledge regarding POUR amongst anesthesiologists.
I spoke with the Perianesthesia Nurse Manager and we agreed that when POUR issues arise, the PACU nurse will always communicate with the surgical team. Also, the order for "patient voiding prior to discharge instructions," will be in the PACU discharge order set, which is written by the surgical team.
T
he biggest discrepancy was among the anesthesia service. 12 out of 17 (70.6%) anesthesia providers assumed patients voided prior to discharge. Whereas, 9 out of 22 (41%) surgical providers assumed the patient voided prior to discharge. After studying the risk management case where the patient was readmitted with POUR, I learned that the nurse was exclusively communicating with the anesthesiologist.
In PACU, the nurse has to decipher if he/she should communicate an issue with the surgical team or anesthesiologist. The vast majority of issues are anesthesia-related, meaning the nurse defers to the anesthesiologist. However, POUR is multifactorial and the biggest contributor to increased risk is the type of surgery. Furthermore, the survey highlighted a lack of knowledge regarding POUR amongst anesthesiologists.
I spoke with the Perianesthesia Nurse Manager and we agreed that when POUR issues arise, the PACU nurse will always communicate with the surgical team. Also, the order for "patient voiding prior to discharge instructions," will be in the PACU discharge order set, which is written by the surgical team.
Click for POUR Pretest
