Swallow Screening Tool
PACU nurses were educated individually prior to the new tool going live in Epic. Each nurse was given verbal step-by-step instructions and followed along by reading the sheet provided by JoAnn DelMonte. To reinforce concepts and address visual learning modalities, PACU nurses were shown screenshots of the new tool and ran through the new swallow screening tool.
See below for instructive material used.
See below for instructive material used.
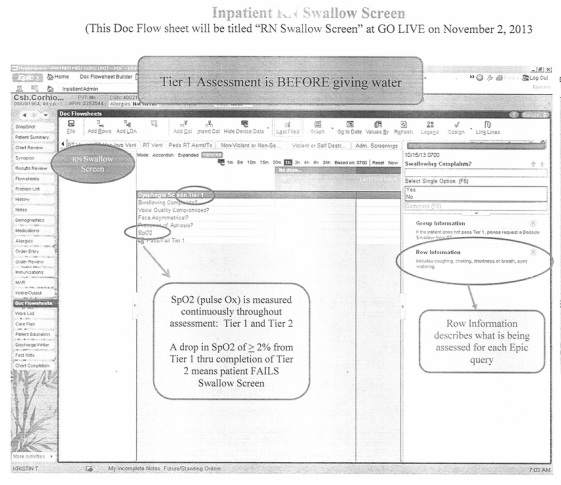
How to perform the RN Bedside Swallow Screening
Begin the assessment with Tier 1
Tier 1
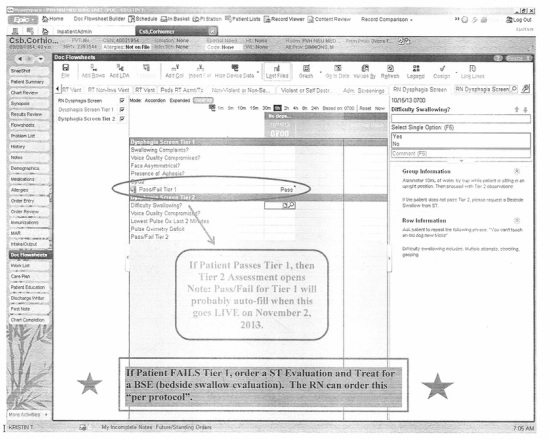
If patient fails Tier 1, STOP- patient needs a SLP consult and must be NPO. RN’s should place an order for “ST evaluation and treat” per protocol.
If patient passes Tier 1, then continue to Tier 2
- Patient must be on bedside pulse ox monitoring continuously
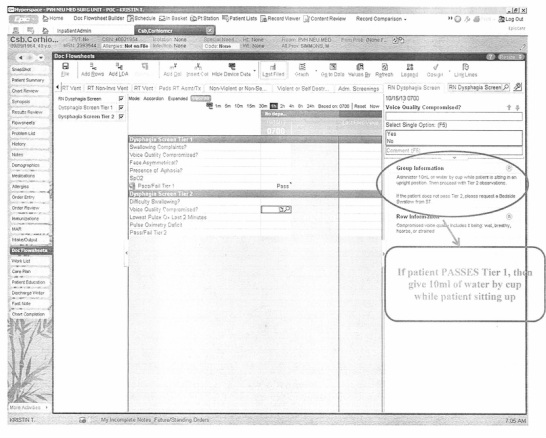
- Patient must be sitting up at 90 degrees
- You will need 1 cup with 10ml of water- no straws
Begin the assessment with Tier 1
Tier 1
- Assess if the patient has swallowing complaints: yes/ no
- Is the face symmetric: yes/ no
- Is there presence of aphasia: yes/no
- Document the SpO2
- Document pass/ fail of Tier 1
If patient fails Tier 1, STOP- patient needs a SLP consult and must be NPO. RN’s should place an order for “ST evaluation and treat” per protocol.
If patient passes Tier 1, then continue to Tier 2
Note:
The following screenshots were created in EPIC SME (or play) environment.
They are not actual patient information.
The following screenshots were created in EPIC SME (or play) environment.
They are not actual patient information.
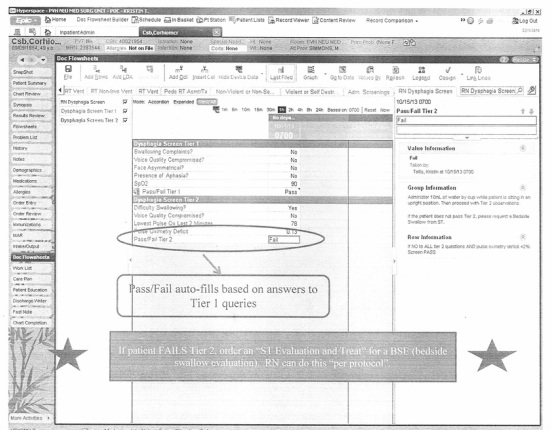
Tier 2
If patient fails Tier 2 STOP patient needs a SLP consult and must be NPO. RN’s should place an order for “ST evaluation and treat” per protocol.
If the patient passes Tier 2 the appropriate diet may be ordered per the physician.
Patient fails the bedside swallow evaluation if:
- Assess swallowing by having the patient drink 10 ml water from a cup-not through a straw. Assess if the patient had difficulty swallowing? Yes/ No (difficulty swallowing is defined as: multiple attempts, choking, gasping)
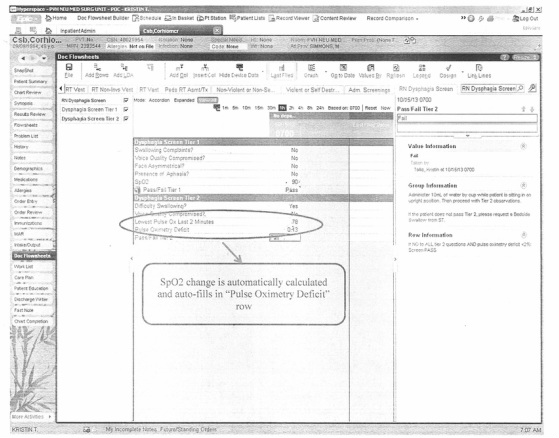
- Ask the patient to repeat a sentence i.e. “you can’t teach an old dog new tricks” and assess if voice quality is compromised: yes/ no
- Document the lowest SpO2 noted over the previous 2 minutes
- The pulse ox deficit will auto populate
- Document the pass/ fail of Tier 2
If patient fails Tier 2 STOP patient needs a SLP consult and must be NPO. RN’s should place an order for “ST evaluation and treat” per protocol.
If the patient passes Tier 2 the appropriate diet may be ordered per the physician.
Patient fails the bedside swallow evaluation if:
- You answer “yes” to any of the questions OR
- SpO2 drops ≥ 2% over the course of the 2 minute post 10ml water administration
- All stroke (and stroke alert) patients must have a bedside swallow evaluation before anything PO- including Aspirin.
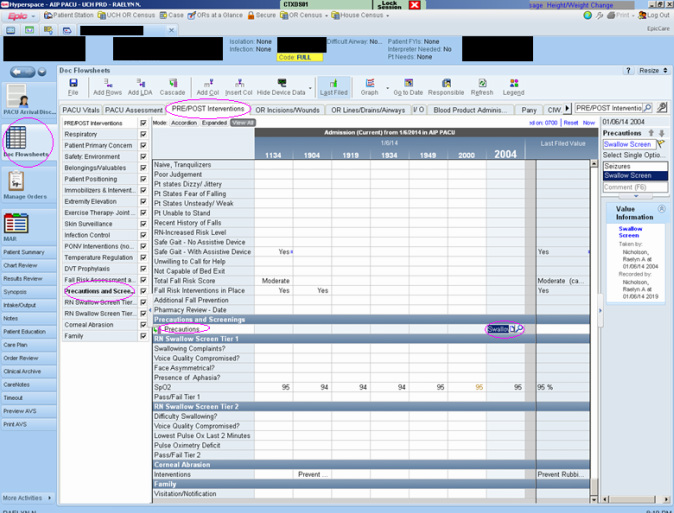
- Document the bedside swallow evaluation in Doc Flowsheets >PRE/POST Interventions >“RN swallow screen”
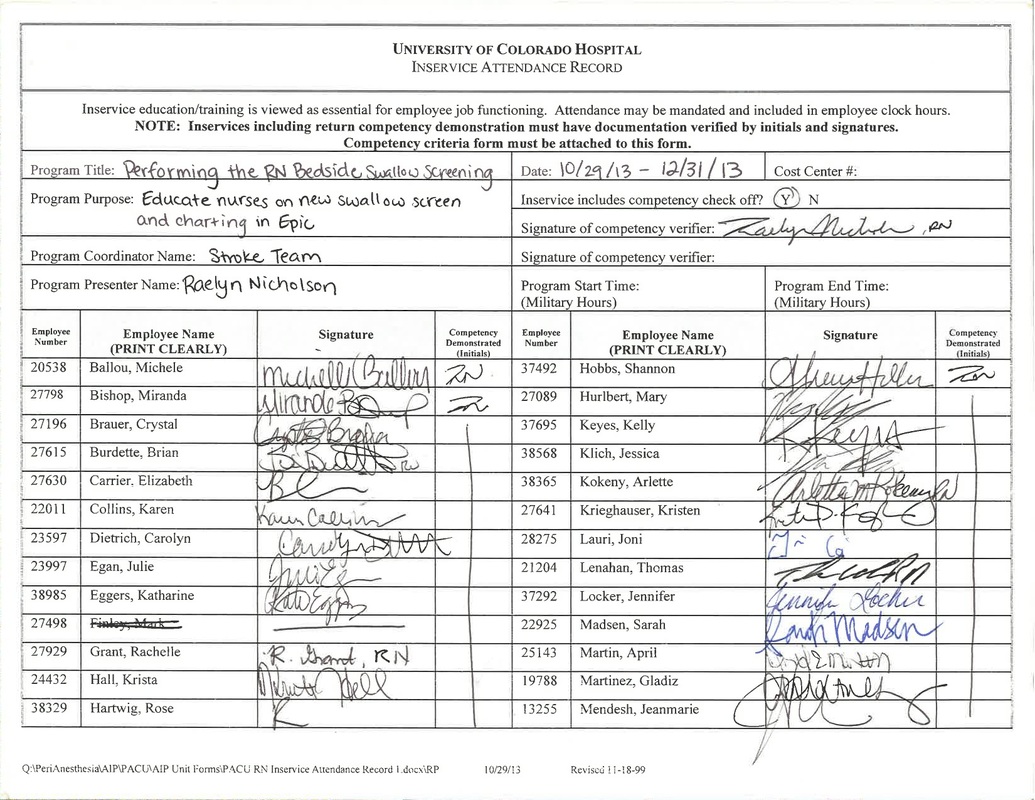
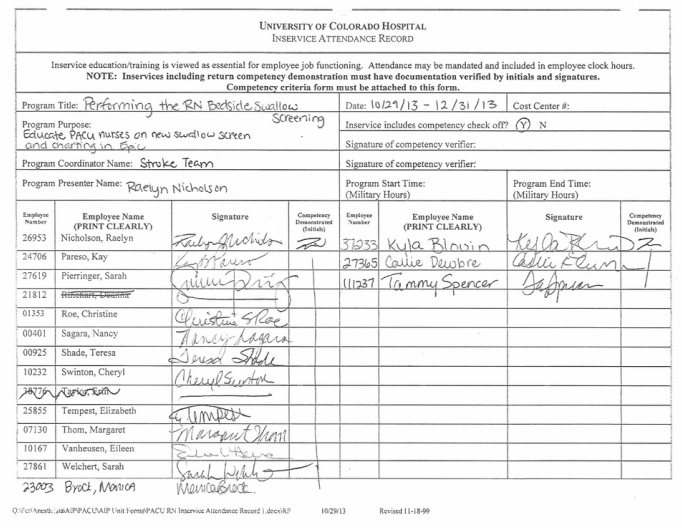
Attendance form signed by PACU nurses
In January 2014, Swallow Screen tool was added to PRE/POST Interventions.
This made the tool easily accessible for PACU nurses.
This made the tool easily accessible for PACU nurses.
Click for Swallow Screening Communication
