Stroke Alert Reeducation
January 21, 2014: PACU had a stroke alert that did not run smoothly, which was attributed to an education gap and miscommunication between the PACU RNs and stroke team.
Situation
14:15 Patient out of OR for simple orthopedic surgery. Patient schedule to be discharged home the day of surgery.
14:59 Stroke alert called by Charge RN due to left sided weakness, aphasia, and difficulty following commands.
The PACU Charge RN asked the Neuro ICU Charge, "How long will it be before the team gets here?" The Neuro ICU Charge responded, "I'm not sure..." Somewhere in that exchange, the Neuro ICU Charge thought the PACU was taking the patient to CT.
After the PACU nurse noticed stroke-like symptoms, she had the PACU charge call the stroke alert. The stroke team went directly to CT while the PACU nurses waited in PACU for the stroke team. After 30 minutes, the PACU charge called the stroke alert line because they were still waiting for the team to arrive. Then she was informed that the team was waiting at CT. During this time, the nurses did not draw labs or complete a blood sugar because they were waiting for orders to be placed. They were also waiting for a CT order and even asked the ortho team to place it. The nurses assumed that they needed a CT order prior to transporting the patient.
Situation
14:15 Patient out of OR for simple orthopedic surgery. Patient schedule to be discharged home the day of surgery.
14:59 Stroke alert called by Charge RN due to left sided weakness, aphasia, and difficulty following commands.
- 14:59 Stroke Alert Page 1: “Stroke Alert:. L side wkness, aphasia, unable to follow commmands. Into OR at 1225, out of OR at 1415. Onset upon arrival to PACU. Pt in stat CT now.”
- 15:08 Stroke Alert Page 2: “Stroke alert pt ------ located in PACU bay 61”
The PACU Charge RN asked the Neuro ICU Charge, "How long will it be before the team gets here?" The Neuro ICU Charge responded, "I'm not sure..." Somewhere in that exchange, the Neuro ICU Charge thought the PACU was taking the patient to CT.
After the PACU nurse noticed stroke-like symptoms, she had the PACU charge call the stroke alert. The stroke team went directly to CT while the PACU nurses waited in PACU for the stroke team. After 30 minutes, the PACU charge called the stroke alert line because they were still waiting for the team to arrive. Then she was informed that the team was waiting at CT. During this time, the nurses did not draw labs or complete a blood sugar because they were waiting for orders to be placed. They were also waiting for a CT order and even asked the ortho team to place it. The nurses assumed that they needed a CT order prior to transporting the patient.
Following the stroke alert, the permanent charge nurse, Eileen VanHuesen approached me and recounted the event. I also spoke with another permanent charge nurse, Mary Hurlburt, who called the stroke alert. After disseminating the information, I emailed the stroke program coordinating nurse (Kimberly Rapp), and explained the situation. See below for the conversation.
After discussing areas of improvement with the stroke program coordinator (Kimberly Rapp), I reeducated staff on stroke alert protocol and the nurse's role. I emphasized what the nurse should do while waiting for the stroke team to arrive and a reasonable timeframe.
PACU Staff Meeting Minutes - 2/10/14 and 2/13/2014
Presented stroke alert reeducation
See page 3 of the meeting minutes
Presented stroke alert reeducation
See page 3 of the meeting minutes
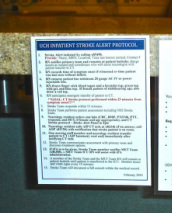
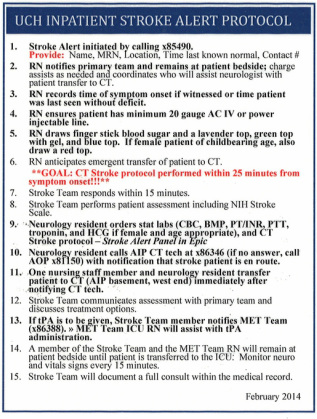
Stroke Alert Protocol posted on charge nurse desk and nursing stations.
PACU nursing staff commented on how crucial the protocol was in guiding interventions and anticipating orders.
PACU nursing staff commented on how crucial the protocol was in guiding interventions and anticipating orders.
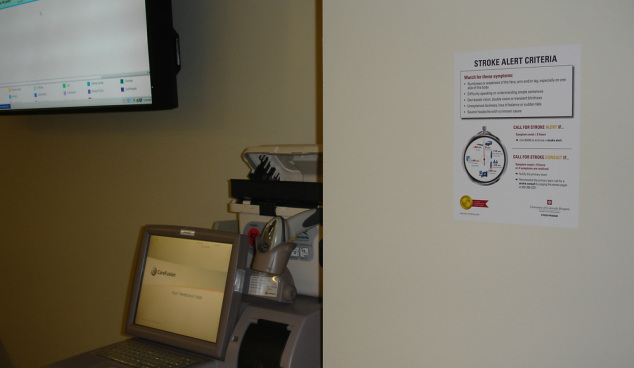
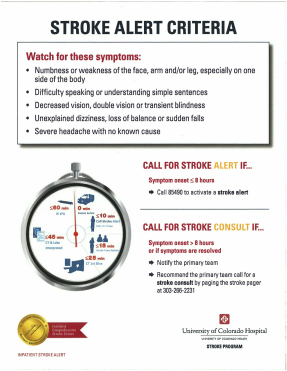
Stroke alert signage posted throughout the PACU.
Evidence of Learning
March 3, 2014
Situation
15: 25 PACU RN returned from lunch. The relieving RN informed her of the patient's mental status change (the patient appeared increasingly difficult to arouse). After reassessment, the patient was not responding to voice or painful stimulus.
15:30 The surgical team arrived at the patient's bedside.
15:35 PACU RN and Charge RN called a stroke alert, stroke panel labs were drawn, and glucose was checked (results were 232).
15:41 Anesthesiologist ordered a stat ECG. Transport monitor on bedside table.
15:45 Stroke team arrived.
15:50 Patient transported to CT. At this time the patient was starting to follow more commands. Stroke team, surgical team, and PACU RN accompanied patient to CT.
16:40 Patient returned to PACU and was oriented to person, place, time, and situation.
16:55 Patient's family were at the bedside.
As opposed to previous stroke alerts in the PACU, the above example was drastically improved. Staff utilized the badge tags and signs posted throughout the unit to anticipate orders and treat the patient. The patient was transported to CT within 15 minutes of calling the stroke alert. In the end, the team concluded that the patient had a seizure.
Situation
15: 25 PACU RN returned from lunch. The relieving RN informed her of the patient's mental status change (the patient appeared increasingly difficult to arouse). After reassessment, the patient was not responding to voice or painful stimulus.
15:30 The surgical team arrived at the patient's bedside.
15:35 PACU RN and Charge RN called a stroke alert, stroke panel labs were drawn, and glucose was checked (results were 232).
15:41 Anesthesiologist ordered a stat ECG. Transport monitor on bedside table.
15:45 Stroke team arrived.
15:50 Patient transported to CT. At this time the patient was starting to follow more commands. Stroke team, surgical team, and PACU RN accompanied patient to CT.
16:40 Patient returned to PACU and was oriented to person, place, time, and situation.
16:55 Patient's family were at the bedside.
As opposed to previous stroke alerts in the PACU, the above example was drastically improved. Staff utilized the badge tags and signs posted throughout the unit to anticipate orders and treat the patient. The patient was transported to CT within 15 minutes of calling the stroke alert. In the end, the team concluded that the patient had a seizure.
Click for Stroke Alert Communication
